TSO is a new drug, taken by mouth, that contains microscopic eggs of the pig whipworm parasite. It acts as a natural regulator of the immune system, by controlling T-cells, a group of white blood cells, and cytokines, signalling proteins that deal with inflammation, among other things.Seems interesting. Reminds me of helminthic therapy -- although doesn't sound like the worms stick around past two weeks. Hints to a lack of diversity of bacteria and other organisms in our gut.
In a pig, the eggs grow into whipworms and reproduce, without causing harm to the animal. In a human, the same eggs live no more than two weeks. But in that time, they appear able to influence the host immune system and stop it attacking tissue and organs.
Showing posts with label Treatment - Pharma. Show all posts
Showing posts with label Treatment - Pharma. Show all posts
Tuesday, August 28, 2012
Pig Parasite To Be Trialled As Treatment For Crohn's Disease
Saw this article about a clinical trial starting to test pig whipworm eggs as a treatment for Crohn's. Here's an excerpt:
Biologics for Inflammatory Bowel Disease Increase Risk for Melanoma
Been a long time since I posted. Came across this article. Here's an excerpt:
Patients with IBD had a higher incidence of melanoma than controls; this association was significant in patients with Crohn disease (incidence rate ratio, 1.45) but not in patients with UC (IRR, 1.13). Researchers observed a trend of increasing risk for melanoma in patients with IBD over time. In a nested case-control analysis, any use of a biologic anti–tumor necrosis factor (anti-TNF) agent was associated with an almost twofold increased risk for melanoma, unlike thiopurines or 5-aminosalicylic acid (5-ASA) medications, for which no associations were observed. The risk for NMSC was increased by almost twofold in patients who used any thiopurine, but was not significantly increased in patients who used anti-TNF agents.Makes sense that there are side-effects of using biologics.
Tuesday, July 13, 2010
Why some people with IBD may not respond to corticosteroids
We all know that corticosteroids are one of the first drugs prescribed to deal with IBD. But it doesn't always work for everyone. Why?
I just came across a press release about new research that uncovered why many people with lupus (another autoimmune disease) do not respond to corticosteroids - or at least steroids in high doses. An excerpt that explains why this is the case:
Currently, those with lupus and other autoimmune diseases, commonly treat the condition with corticosteroids to suppress their overactive immune system and prevent it from attacking healthy tissues which can result in symptoms such as inflammation, pain and organ damage.
These steroid treatments work by killing certain immune system cells, including plasmacytoid dendritic cells (PDCs) that overproduce type 1 interferons, an immune system substance that contributes to lupus and other autoimmune diseases. However, unlike other conditions, steroid treatments are not as effective against these cells in those with lupus.
By largely studying children with systemic lupus erythematosus (SLE), BRI scientists in collaboration with scientists at Dynavax in Berkeley, CA, were able to solve the mystery behind the resistance. They determined that two immune system proteins known as toll-receptor 7 (TLR7) and toll-receptor 9 (TLR9), cause an activation of PDCs—the very cells steroids target—negating the effects of treatment. BRI scientists reported their findings in the June issue of the journal Nature.
A similar resistance mechanism might be at play with people with IBD (and other autoimmune diseases). It hasn't been proven yet obviously, but it's certainly something to consider when you're working with your doctor to deal with a serious flare-up. The traditional prednisone or budesonide (Entocort) may not work for you simply because your body works against the mechanism of the drugs.
Thursday, July 8, 2010
Two new drugs that could be used for autoimmune and inflammatory diseases
Saw two recent articles about new drugs that could be used to treat autoimmune and inflammatory diseases, including multiple sclerosis, inflammatory bowel disease, arthritis, and others.
The first article was about a cancer drug, bortezomib, that was used in an animal study to treat inflammatory disease. The cancer drug induced cell death in only the harmful (active and proliferating) T-cells.
The second article was about a new protein from Compugen called CGEN-15001 that was found to abolish recurring relapses of multiple sclerosis in an animal study. The protein also delayed the onset of the disease. The protein apparently has some effect on the regulatory pathways in the immune system.
Both seem pretty interesting.
Monday, June 21, 2010
Prostaglandin D2 a potential treatment for Ulcerative Colitis
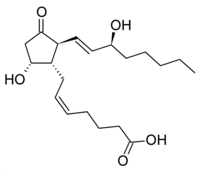 A recent study may suggest a new treatment for ulcerative colitis. The study, to be published in the journal Proceedings of the National Academy of Sciences, found that people with ulcerative colitis that have been in remission for a long time-period have higher levels of Prostaglandin D2 than those that don't. It's unclear whether the higher levels of the chemical are a result of being in remission or the cause of the remission, but the study is interesting nonetheless as it suggests follow-on research.
A recent study may suggest a new treatment for ulcerative colitis. The study, to be published in the journal Proceedings of the National Academy of Sciences, found that people with ulcerative colitis that have been in remission for a long time-period have higher levels of Prostaglandin D2 than those that don't. It's unclear whether the higher levels of the chemical are a result of being in remission or the cause of the remission, but the study is interesting nonetheless as it suggests follow-on research.
FDA requires cancer warning on TNF blockers (old news)
I definitely see the value of these drugs in the short-term to help get the inflammation under control, but long-term use doesn't seem like a solution. (Hence why I'm avoiding them!)
Thursday, June 17, 2010
Why Pregnancy Pushes Autoimmune Diseases into Remission
 A friend of a friend of mine has had Crohn's for many years. But when talking to her, she mentioned that during her pregnancy all her Crohn's symptoms completely subsided and she was in "remission". Why? This apparently is a common phenomenon for pregnant women with autoimmune diseases -- during pregnancy their diseases go into remission.
A friend of a friend of mine has had Crohn's for many years. But when talking to her, she mentioned that during her pregnancy all her Crohn's symptoms completely subsided and she was in "remission". Why? This apparently is a common phenomenon for pregnant women with autoimmune diseases -- during pregnancy their diseases go into remission.A new study from the University of Michigan may explain why. Apparently the expression of an enzyme called pyruvate kinase is reduced in immune cells in pregnant women. The reduction in this enzyme "dials-down" the immune system supporting the acceptance of the fetus.
An excerpt from the article:
In his search to explain the phenomenon, Dr. Petty knew to look for a metabolic pathway ormechanism with two characteristics. It had to "dial down" the intensity of the normal immune response, an action needed so that a pregnant woman does not reject the fetus, which has proteins from the father that are "foreign" to the mother. At the same time, such a mechanism must support cell growth needed by the developing fetus.
The activity of the enzyme pyruvate kinase–and its product, pyruvate–fills both roles: promoting cell growth while modifying the immune response. Because pyruvate kinase activity is depressed duringpregnancy, cell metabolism supports an increased production of lipids, carbohydrates, amino acids, and other substances that support cell growth.
This suggests an interesting alternative therapy or treatment option for the future (and I'm not suggesting that you just go get pregnant!). There may be a way to use this immune pathway in a drug therapy. It doesn't necessarily identify or address the root cause of IBD, but it could lead to another alternative therapy.
Thursday, May 6, 2010
Anti-TNF Decreases Presence of MAP
Thursday, December 24, 2009
A Potential Stem Cell Treatment for IBD from Pfizer


Pfizer announced some news this week that could result in a stem cell treatment for inflammatory bowel disease (IBD), including Crohn's. On Monday, Pfizer struck a development and commercialization agreement with Athersys, Inc., a Cleveland biotech company. Pfizer plans to develop a therapy for IBD based on MultiStem, the Athersys adult stem cell product line.
From reading through the MultiStem website, the product seems to have great potential as a therapy. The really dumbed-down version of the therapy (I'm a dummy, so correct me if I'm wrong) would be to inject these cells into a sufferer of IBD and then the cells, based on the
local environment and specific type of inflammatory response, would produce molecules to help properly regulate the immune system. The stem cells would not be a permanent solution. Similar to other biologics (e.g. Cimzia), they would have a temporary impact on how the immune system functions and to continue to see benefits you would need to continue to take the drug. Here's an excerpt:
MultiStem consists of a special class of human stem cells that have the ability to express a range of therapeutically relevant proteins and other factors, as well as form multiple cell types. Factors expressed by MultiStem have the potential to deliver a therapeutic benefit in several ways, such as the reduction of inflammation, protection of damaged or injured tissue, and the formation of new blood vessels in regions of ischemic injury. These cells exhibit a drug-like profile in that they act primarily through the production of factors that regulate the immune system, protect damaged or injured cells, promote tissue repair and healing and most or all of the cells are cleared from the body over time.
The real unique thing about MultiStem versus other biologics is that it could actually have multiple methods of working (the beauty of stem cells). Here's an excerpt:
Though the cells have the potential to differentiate into a variety of cell types, in certain indications the primary mechanism of MultiStem appears to be the production of a physiologically relevant and complex set of therapeutic molecules in response to the local environment. In the initial indications Athersys is pursuing, the cells appear to minimize the inflammatory reaction that occurs in response to ischemic events (such as myocardial infarction or stroke) or the anti-host immune reaction seen in graft vs. host disease (GvHD), and promote healing and recovery. Unlike traditional pharmaceuticals, MultiStem cells are dynamically regulated, and have the potential to respond to signals of inflammation or tissue damage in multiple ways. Potential mechanisms of benefit include protection of damaged or injured cells, reduction of inflammation, stimulation of new blood vessels, and the recruitment of other cell types to promote tissue repair and healing.
Athersys claims that one of the benefits of the drug is that it can be scaled to be produced efficiently on a large scale. That could mean the drug could be made available to people on the same scale that traditional pharmaceuticals are. (Although I wouldn't expect the scale economies to translate into affordable prices).
Great news and looking forward to see what Pfizer brings to market. And in terms of bringing the product to market, here's a good excerpt from The Motley Fool ("Pfizer Swings for the Fences"):
MultiStem is being tested in several conditions, but Pfizer's license is specifically for the treatment of inflammatory bowel disease (IBD), a group of conditions that includes ulcerative colitis and Crohn's disease. The license is only costing Pfizer $6 million up front because the technology is still relatively unproven, having not entered clinical trials for IBD yet. Athersys can get milestones of up to $105 million and royalties as the drug passes through clinical trials and is commercialized.
Pfizer will pay for the phase 1 and 2 trials. Then, if it gets that far, Athersys will have the option of co-developing the drug -- sharing profits and losses -- or letting Pfizer proceed on its own and take the milestones and royalty payments.
Unlike traditional stem cell companies like Geron (Nasdaq: GERN) that are developing stem cells to regenerate tissue, MultiStem uses donated bone marrow cells to produce a product that promotes healing of the tissue through cell signaling. Essentially it has a more drug-like profile as the stem cells are cleared from the body.
So certainly a ways out.
Thursday, October 29, 2009
Anti-TNF Drugs Don't Seem to Increase Cancer Risk
Good news for those that use TNF-blockers to manage their Crohn's disease. Long-term use of the drugs (at least for 6 years or less) does not appear to increase your risk of cancer. That's certainly a concern as TNF is part of the body's immune response in dealing with "tumor"-like cells. The study looked at both short and medium term use of these drugs for rheumatoid arthritis and didn't find any elevated risk of cancer.
UPDATE: (6/21/2010) - The FDA released a cancer warning for TNF-blockers back in August 2009. See this related post. Thanks to the anonymous person that commented!
Subscribe to:
Posts (Atom)